Complications Associated with the Placement and Restoration of Dental Implants
Case Report 1
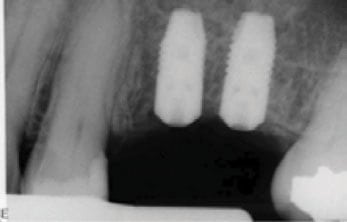
Patient was a 55-year old male who presented for treatment that included the placement of 2 implants in the maxillary left upper quadrant. Pre-operative radiographic examination included a peri-apical image as well as a panoramic radiograph (Figure 1). It was noted that the patient needed a sinus elevation procedure along with implant placement. An internal sinus elevation procedure with simultaneous implant placement was planned. It was decided to place one 4.0 mm platform implant and one 3.5 mm platform implant due to space availability.
Upon placing the 3.5 mm implant in the #14 region it was noted that the implant had moved sub-crestally and was about 3 mm below the crest of the bone (Figure 2). Upon attempting to engage the implant, the implant continued to move in an apical direction and was soon not visible (Figure 3). A panoramic radiograph indicated that the implant was lodged in the maxillary sinus (Figure 4).
The patient was then re-appointed for a Caldwell-Luc approach (Figure 5). A second panoramic radiograph taken on the morning of the procedure indicated a more coronal position of the implant in the maxillary sinus. Following a vestibular incision apical to the left maxillary canine, an opening was made into the maxillary sinus. Placement of a suction tip into the sinus immediately retrieved the implant (Figure 6). The incision was subsequently sutured and the patient healed uneventfully. Following approximately a 3-month period, the patient was re-appointed and a 4.0 mm platform implant was successfully placed in the site (Figure 7). The patient is currently getting ready for the restorative phase of treatment.





Implants Lodging in the Maxillary Sinus
Reports of foreign bodies being displaced into the maxillary sinus as an outcome of treatment procedures have included objects such as teeth, roots, impression materials, dental instruments, broken burs and, more recently, dental implants [13]. Implants have been reported to being displaced into the maxillary sinus during various steps of implant placement and restoration. Reports of implant displacement have been made during the time of implant placement, at the uncovering appointment, when connecting the abutment, and during the retrieval of failed implants. They have also been reported to migrate into the sinus following implant placement.
Implant placement in the posterior maxillary quadrants has become a routine treatment option. However, due to the pneumatization of the maxillary sinuses usually associated with tooth loss, placement of implants in the region usually involves either internal sinus elevation procedures or lateral window procedures. Implants are placed either at the time of the sinus elevation procedure or placed following a healing period that can range from 3-6 months. Implants are placed at the time of sinus elevation when at least 4-5 mm of crestal bone is present [14, 15, 16].
While this complication was seen more often when cylinder implants were used, screw-form implants have also been reported to have become lodged within the maxillary sinus either at the time of placement or following implant placement [17]. Cummings et al [18] reported that a critical review of the literature from 1990 to 2007 found ten reported cases of implants displaced into the maxillary sinus, and one case in which the implant was displaced into the nasal cavity. They commented that the documented number of incidents was almost certainly far below the number of actual occurrences due to the fact that not all cases get reported. The authors also noted that in all these cases, parallel wall implants were placed.
While implants being lodged in the maxillary sinus at the time of placement can be understood, the complication of implants migrating into the sinus after several years has also been reported [15, 16]. The different mechanisms to explain this complication include; changes in intrasinal and nasal pressures; auto immune reaction to the implant, causing peri-implant bone destruction and compromising osseointegration; and resorption produced by an incorrect distribution of occlusal forces [17].
